Letter to the school board, local health board, attorney general Eric Schmitt, Governor Mike Parsons, and like minded community members and concerned parents
danagranbergnillmdfaafp.substack.com
Letter to the school board, local health board, attorney general Eric Schmitt, Governor Mike Parsons, and like minded community members and concerned parents
The Urgency of Normal Toolkit, Mask Mandates, "Vaccine" coercive messaging
Letter to the school board, local health board, attorney general Eric Schmitt, Governor Mike Parsons, and like minded community members and concerned parents
In May 2022, I received an email from Attorney General Eric Schmitt that referenced a “toolkit” to be used by “parents, students, mentors, teachers, and administrators for advocacy for our children and an urgent return to normal.” The latest version of the toolkit is located at urgencyofnormal.com. (1)
One of the points highlighted in the toolkit is: “Maintain in-person learning regardless of case counts and vaccination rates.” (1)
The mental and emotional cost of COVID-19, as well asthe response measures that were implemented, is undeniable. (1) Although in-person learning is an admirable goal, it should not be used to implement policies that have proven ineffective, harmful, or discriminatory.
In the last 1.5 years, masking, tracing, quarantines, and testing have often targeted the “unvaccinated,” despite such measures not being scientifically justified. (1) School boards have communicated that COVID-19 policies were heavily, if not exclusively, based on recommendations from the local county health boards and/or CDC recommendations. Even though CDC guidance resulted in policies that often failed to reflect the reality of emerging observations and data, financial incentives and other factors impacted compliance—despite increasing numbers of parental objections and concerns expressed at school board and health board meetings. (5,10)
Financial incentives for implementing and complying with CDC-based policies was evident through programs such as the CRRP Act (ESSER and GEER funds) and seemed to offer parents little hope of push back—even when equipped with evidence to support their concerns. (15) Concerned parents have mobilized to make sure that financial incentives do not unduly influence implementation and compliance of COVID policies. One recent Facebook post expressed such sentiment: “Last night, the Hazelwood School District voted to mask kids back up when school starts next month. Hazelwood was in the top 3 for most federal COVID money received out of 500+ school districts in the state. They received more than 30 million dollars. They sold out the children in their district.” (32) School boards and health boards could plead ignorance during the early COVID chaos while implementing CDC recommendations despite parental pushback, but to continue the same policies nearly two years later with solid data that such policies are both ineffective and harmful is indefensible.
In addition to the financial influences, there was suppression of information that was important in providing proper informed consent. Documents released through the FOIA in late July (after the CDC was sued by America First Legal) raise questions about how the CDC utilized social platforms to propagate “safe and effective” messaging while it censored, restricted, and labeled (as misinformation) any conflicting medical data or opinions. (24) Given some of the recent legal wins for those financially, physically, or otherwise harmed by schools, hospitals, or military policies, it is my hope that this is the beginning of a domino effect of legal actions to hold the CDC, organizations, and individuals accountable for continued implementation of failed or unethical and discriminatory policies (25, 26, 27, 29). Given that “vaccine” manufacturers as well as the CDC have both admitted that these injections do not prevent contraction or transmission of COVID-19, any policy treating “unvaccinated” individuals differently is nothing more than discriminatory and punitive.
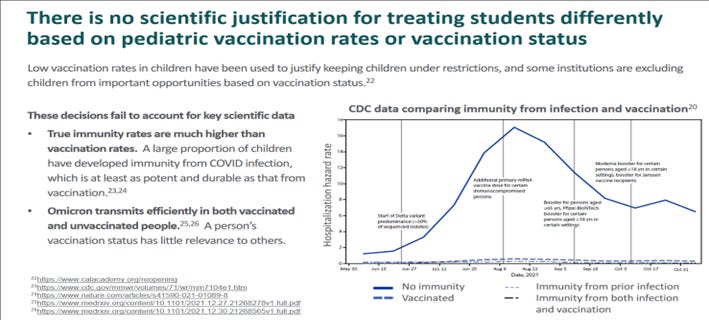
When the COVID-19 “vaccines” were not shown to prevent infection or transmission of COVID-19, the CDC chose to change the definition of a vaccine rather than admit this fact. The CDC (and health departments, school boards, etc.) continued to implement policies (for both students and staff) that focused on “vaccinated” vs “unvaccinated” statuses despite knowledge that both contracted and transmitted the virus. Despite efforts to suppress previously documented science on the importance of natural (acquired) immunity, studies have once again confirmed (and is demonstrated in the toolkit) that acquired immunity is as good, if not superior, to COVID-19 injections. (20,21) No (asymptomatic) person should have to be continually retested or coerced into receiving COVID-19 injections under any circumstances, but especially if they have acquired immunity (20, 21).
Mandating policies for all children despite known risks of some of these policies, will continue to draw ire from parents that also want to protect their children-from the effects of prolonged masking, unproven and unreliable PCR testing, unequally applied tracing and quarantines and coercive “vaccination” messaging. It appears that the path forward is through legislation and litigation given other efforts have proven ineffective. For example, medical and religious exemptions were denied by many schools (and employers) which left many with no choice but to comply or face financial and other consequences.
In January of this year, I read a blog in my American Family Physician journal by Dr. Jennifer Middleton that detailed the CDC’s Test-To-Stay (TTS) Strategy defined as:
“...a practice comprised of contact tracing and serial testing to allow school-associated close contacts who are not fully vaccinated to continue in-person learning during their quarantine period. While implementation of TTS may vary, contact tracing and testing as well as masking of contacts during their in-school quarantine period are integral to minimize risk of transmission.” According to the article, “TTS is only necessary for unvaccinated children, but vaccination rates for children aged 5-11 years in the U.S. remain quite low... So, TTS may continue to be needed for the foreseeable future”. (2)
The panelists who produced The Urgency of Normal toolkit penned an open letter to the CDC which can be found at urgencyofnormal.com. The letter proposes a “test to treat” approach. While the focus is on high-risk (immunocompromised) children rather than “vaccination” status, it also states that one of the ways to focus on these high-risk individuals is by “encouraging vaccination” and “making prophylactic treatments (Evusheld) and early treatment (Paxlovid and monoclonal antibody therapy) widely available.” It’s interesting that only expensive and experimental agents (authorized for emergency use) and without known efficacy or safety data are the treatments of focus mentioned by the panel. (12) A review by the Front Line COVID-19 Critical Care Alliance summarized findings from 27 studies on the effects of ivermectin for the prevention and treatment of COVID-19 infection, concluded that ivermectin “demonstrates a strong signal of therapeutic efficacy” against COVID-19 (19). Another study showed a 92% reduction in COVID-19 mortality rate with regular use as prophylaxis. (28) Yet another example, Nitric Oxide Nasal Spray (NONS): A Lancet study showed NONS blocks entry into nasal passages and lowers COVID viral load by 94% in 24 hours. (18) The panel also encourages “vaccination” for high-risk individuals despite emerging data that now suggests that booster shots might “adversely affect the immune response” and that “COVID 19 vaccination is a major risk factor for infections in critically ill patients” (22).
Despite data that contradicts the pro-“vaccine” bias, the echo chamber continues at the state and local levels regarding the no-risk, all-benefit “vaccine” messaging. For example, as of August 1st, 2022, the Missouri Department of Elementary and Secondary Education website has the following posted statements on its website (16):
“Vaccination is the best way to protect children aged 5 and older from COVID-19.”
“The vaccine is safe and effective.”
The Missouri Department of Elementary and Secondary Education (DESE) also provide links to other resources with similar messaging. For example, a link to the “COVID Vaccine Toolkit for Missouri Schools” produced by the Missouri Chapter of the American Academy of Pediatrics. (18) There are thousands of health professionals who argue that the safety and efficacy of these (experimental) “vaccines” is not justified, especially in the pediatric population. None of the sources that appear on the Missouri DESE website appear to offer any professionals or organizations that provide a more balanced risk-versus-benefit discussion of these injections.
The Urgency of Normal toolkit rightly points out: “There is no scientific justification for treating students differently based on pediatric vaccination rates or vaccination status.” (1)
Despite this statement, the CDC and many in the medical and school communities continue to advocate just such an approach. The point of having different policies for “vaccinated” vs. “unvaccinated” children coerces parents into vaccinating their children to avoid the inconveniences, restrictions, and differential treatment imposed on the students & family. (3)
In August of 2021, Missouri’s Governor Parsons stated, “At some point the people that have had the vaccine, that have had COVID, that have been tested for antibodies and they’ve got it in their system, I think that there needs to be a division between those people and the people who are unvaccinated.” What type of “division” does Governor Parsons feel is appropriate? This statement has not aged well, yet the damage done by this type of divisive, discriminatory, non-science-based rhetoric is not to be underestimated. Perhaps this type of rhetoric will help efforts to justify vaccine passports or contribute to the exclusion of “unvaccinated” Missourians from opportunities such as study abroad, a night at the Kauffman center, or even applying for your driver’s license without a mask. (Appendix) What this type of rhetoric will not do is help mitigate COVID transmission in Missouri, given the “vaccinated” (and boosted) are not only contracting and transmitting COVID virus (and variants), but also being hospitalized and dying from the virus. The virus does not discriminate, so why should our governor, government, and schools?
In the entirety of the Urgency of Normal Toolkit, there is no mention whatsoever of the risks of the mRNA gene therapy injections (“vaccines”). Given the inherently low risk of COVID morbidity and mortality for healthy children, the risks are of paramount concern as this population reaps little to no benefit from these injections. As the Urgency of Normal Toolkit consistently highlights the presumed benefits of these injections, an equal effort should be made to acknowledge emerging safety concerns (such as myocarditis), lackluster and short-lived efficacy, and unknown or long-term risks of gene therapy injections in developing children, increased all-cause mortality, marked increase in cases of Sudden Adult Death Syndrome (SADS), menstrual irregularities, neurodegenerative and hematologic disorders, just to name a few. The Urgency of Normal Toolkit highlights that it was created “to make evidence-based decisions for pre-K and K-12 schools and extracurricular activities” and “summarizes the most important data regarding COVID and children of all ages so you can be empowered.” Such empowerment will not come from highlighting (marginal) benefits for children while failing to present the risks to parents, or at a minimum acknowledging the lack of data to support the safety and efficacy and long term considerations of these injections.
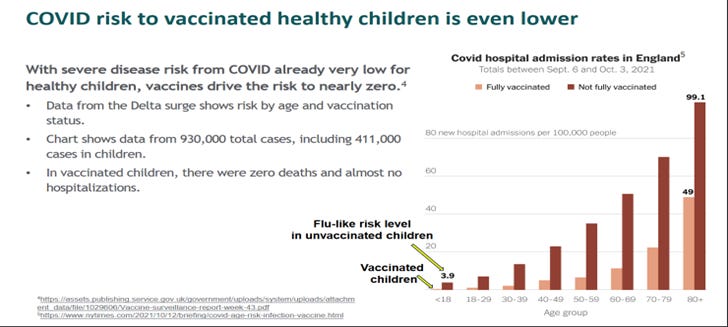
The following (ToolKit Graph 1) implies there is reduction of severe disease and hospitalization for “vaccinated healthy children” (despite an already very low risk). Given the reduction appears minimal, the significance (if any) needs to be clarified by the panel. Please note the slide also depicts “fully vaccinated” and “not fully vaccinated” during a very small snapshot of time from 9/6/21 to 10/3/21. Given these factors, what is the relevance of this slide? Why differentiate and highlight the difference between these two groups given the minimal significance noted? Why are older individuals (which are not the focus of the Toolkit) included in the graph? Does “not fully vaccinated” include “partially vaccinated” individuals? If so, this would seem to further diminish the attempt to prove the point that “COVID risk to vaccinated healthy children is even lower.” This study was also less than a month! Perhaps selecting a study that has longer duration and demonstrates how “vaccinated” students fare months later as these injections will likely not be effective with variants and may impact the susceptibility to variants. Unfortunately, these children are now in a clinical trial for which only time will tell if the benefit of treating an illness with a statistical zero percent mortality for healthy children warranted the risk of an untested, mRNA gene therapy agent with unknown safety, efficacy and long-term consequences.
TOOLKIT Graph 1
Though the ‘Urgency of Normal’ is suggesting that “vaccination” is beneficial for healthy children, I would argue it’s not supported by emerging safety and efficacy data, VAERS, vaccine injury (congressional and social media) testimonials, reinfection rates (especially for those who are boosted). Data is emerging now some of which directly contradicts this information with regard to both COVID hospitalization and death. Perhaps a pause in this type of messaging should be considered until further studies can validate if immune suppression and increased susceptibility to variants is higher in “vaccinated” and boosted individuals.
The way medical information is collected and presented for parents is of utmost importance in communicating very complex medical data in an ethical and efficient manner. By highlighting only studies that support a “pro-vaccine” message while not presenting data that shows concerning safety signals, parents are unable to make an informed “evidence-based decision.” Nor does it allow open discussion and debate of all factors necessary to truly lower the negative physical, mental, and emotional impact of COVID-19.
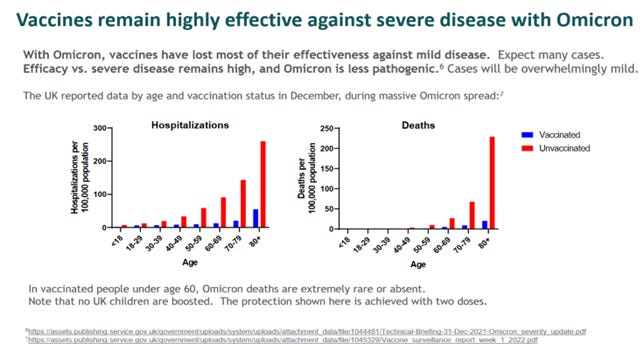
This toolkit slide below (Toolkit graph 3) highlights reduced hospitalizations and no reduction for death in school-aged children while stating that the “protection here is achieved with two doses” noting that “no UK children are boosted”. The study was during the month of December 2021 only. Does the panel have access to UK data and studies that include children that are boosted? Given some of the concerning signals noted with waning immune function with repeated injections or boosters (20, 21), a more robust timeframe would be of benefit given there is minimal (if any) statistical significance to the hospitalizations and no reduction in deaths for the age 18 and under groups. Again, I wonder why this slide was included with minimal significance apparent for the Pre-K to 12 student groups the toolkit is intended.
TOOLKIT Graph 3
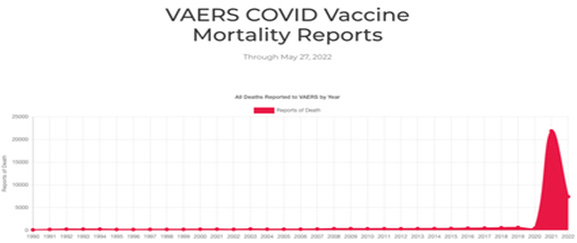
The recommendations to proceed with mRNA injections in children has many considerations that are different than adults and the elderly. By blending adult and elderly data with a “pro-vaccine” slant, it skews the data to appear that there is more benefit than supported in the data for individuals 18 or younger. The toolkit stresses that there is no reason to treat a “vaccinated” child different than an “unvaccinated” child, yet the toolkit does just that throughout the presentation—with no compelling data to justify doing so. Highlighting the smallest of perceived benefits in graphs without mention of emerging adverse effects documented in VAERS (Graph 4) and other sources does not fully inform the community.
Despite “100% safe and effective” narratives which were the initial messaging, Pfizer and the FDA had to be ordered by a court to release safety and efficacy data that they wanted sealed for over 50 years. (23) This is not an ethical way to inform the public or implement public policy, nor does it enable anyone to “follow the science.” When examining just some of the details that have been made available through the monthly court ordered document dumps, it is an understatement to say that what the documents reveal is unsettling and should be considered by parents in the decision-making process. Has the panel reviewed the pages of side effects of special interest listed by Pfizer early in the trials? Has the panel reviewed any of the court ordered “document dumps” each month to ensure that they are reviewing all data that could be relevant to those seeking information on these injections? Is the panel following FDA hearings and testimony as these products continue to be approved for younger and younger age groups? Do any members of the panel have any conflicts of interest to disclose (it was not present in the toolkit)?
Graph 4
The “pro-vaccine” overtones in the toolkit also extends to adults, which are not the subjects of the ‘Urgency of Normal’ toolkit. Again, an all-benefit, no-risk approach in the presentation is apparent and two examples are highlighted:
Example 1: “De-escalate fear around getting COVID. Talk openly with children about how safe they are, and how well vaccination protects the adults in their lives.”
Example 2: “Encourage a booster dose for parents, caregivers and school employees if older or in higher-risk groups”
Below is one chart of many that I could present for a consideration that challenges the toolkits assertion that “vaccination”/boosters decrease COVID hospitalizations and death. Graph 5 depicts increased COVID-19 deaths increasing after vaccination in Uruguay (9). There are similar graphs from other countries as well that highlight the need to continually reassess emerging data, especially if it contradicts messaging. Other graphs showing similar results to Uruguay in highly “vaccinated” countries are available to the interested researcher (9).
Graph 5
In one of the first toolkit slides, the stated goal was “to inform you with accurate data, give it context you can understand, and provide guidance about confusing issues. … and (to) provide this data to support every community in making their own decision”. Information should address both benefit and risk. I do not want to deviate from the focus on the children, but these statements deviate from the stated purpose of the toolkit. If the toolkit is aimed at the pre-K through 12 group, why is “vaccination” for adults repeatedly addressed and promoted?
If the panel was going to extend data and recommendations into any age group, it should have been into the college and young adult age group (under 30). Many students face discriminatory policies in their colleges and professional training or deal with policies that are coercive in nature. Like pre-K through 12, healthy young adults also have very low risk-near zero- of COVID-19 morbidity and mortality (as evidenced by the toolkit slides).
Incentives for “vaccinated” students at my daughter’s college this fall ranged from free t-shirts and donuts to drawings for tuition, iPads, and other prizes. Only “vaccinated” students were eligible. Denying “unvaccinated” student participation in certain activities and the peer and social pressures created by divisive and medically inaccurate messaging and policies is discriminatory, punitive, and unnecessary. For both the fall and spring semesters, my daughter had to be tested, despite being asymptomatic. A test-exemption request was denied by her college upon return for the spring semester, even though this test was no longer even approved by the FDA for emergency use authorization! In addition, the college was fully aware (and acknowledged in writing) that “vaccinated” students were both contracting and transmitting COVID-19. Although asymptomatic, she tested positive in January upon her return to college for the spring semester and spent 5 days in what could only be described as solitary confinement. Three weeks after her positive test I received a letter with instructions from the health department on what to do with the “positive result” to “protect others.”
Any CDC type “Test to Stay” policy that divides “vaccinated” from “unvaccinated” individuals is not only not medically or scientifically justified, but it is not ethically sound. We still have work to do locally and nationally (Appendix 1) given the CDC (and those who adhere to their guidelines) continue to push failed policies and divisive messaging. This unfortunately includes Missouri Governor Mike Parsons as referenced earlier.
Many have advocated that natural immunity has likely developed in many healthy young people and the toolkit’s graph below demonstrates the fact that natural immunity is at least (if not more) as protective than “vaccination.” Given this information—and a near zero statistical risk of COVID-19 death in healthy children and young adults to begin with—a more balanced discussion is needed if “vaccines” are going to be encouraged despite lack of safety and efficacy data. In Governor Parson’s statement, he references those that “have been tested for antibodies and they’ve got it in their system”. If this was a genuine interest in natural immunity by the government, schools, and the medical establishment, there would have been information and resources to accommodate these needs. This was not the case.
TOOLKIT Graph 6
Prolonged Face Masking (Mandates)
The risks of prolonged face masking needs further study, especially given the ineffectiveness shown in numerous published articles. Parents must be informed of the risks associated with masking children, especially when no benefit has been shown in reducing transmission. While the toolkit demonstrates that the studies used by the CDC to justify their recommendations were unable to validate the benefit of mandated masking, it does not go far enough in questioning why the CDC (and others) continue to push this approach despite these concerns.
We cannot discount the possible harms to our children’s immune systems and overall health from such constant and prolonged use of masks. We have no prior experience on the subsequent outcomes pertaining to children’s development, health, and well-being from prolonged masking. (2)
Some of the presentations made to the health and school boards over the last 2 years cited a few of the following concerns from forced mask wearing (4):
Reduced O2 levels (unknown effect of prolonged O2 deprivation)
Increased CO2 levels-prolonged exposure to levels that exceed “permissible CO2 content” (10)
Repeated touching (and misuse) of a device meant to “filter” disease
The Foegen effect: Mechanism by which the re-inhalation of hyperdense droplets “trapped” in the mask can INCREASE case mortality of COVID-19 (7)
Short-term and long-term psychological effects of prolonged mask wearing
Social and language development delays given children cannot “read” faces (10)
Other diseases can emanate from damp/hot mask environments (skin or respiratory infection)
Psychological effects of prolonged mask wearing (pediatric mental and emotional health)
Newer concerns such as respiratory implications of breathing in microplastics and other materials from masks (6,8)
Environmental cost of inappropriate disposal of billions of masks
These are matters too important to disregard. The consequences could be significant and lifelong, especially for our children. (6) Those persisting in efforts to promote mandatory prolonged mask wearing for our children will need to account for these concerns and any data that continues to emerge if they choose to ignore the recommendation to make masking optional policies. Numerous studies that have demonstrated the health concerns of prolonged masking were summarized by Dr. Paul Alexander. (4)
Several times in 2021, parents presented studies to our local health and school boards that demonstrated negative consequences of prolonged masking of children. When there is risk involved, there should be choice. There are also sources other than the CDC that should be involved in implementing ethical, scientifically supported solutions.
Despite studies showing that masking does not work and can cause significant harm, the CDC continues to recommend policies for K-12—with no regard to these factors (11).
The most important mask recommendation from the toolkit is: “Moving to mask-optional policies and an immediate end to mandatory masking.”
Test to Stay (TTS) would violate this recommendation if implemented. In addition to the studies listed in the toolkit, there are many mask studies that show harm with prolonged masking, some of which were referenced and presented to the Clay County Health Board and/or the North Kansas City School Board. (4,6,8)
Our children being subjected to mandates and policies on masking, testing, tracing, and isolation and quarantine, as well as coercive messaging (and for some, mandates) regarding the experimental mRNA gene therapy inoculations is an example of what happens when politics, money, power, fear, groupthink, bias, and censorship dictate public health policy rather than an ethical, measured, data-driven, science-based approach. I am hopeful that the toolkit’s panel requests that these issues be discussed with “openness and mutual respect” to allow communities to “make their own decisions.” (Appendix)
The pro-“vaccine” overtones are not appropriate in the toolkit given the increasing data emerging. The risks of experimental gene therapy mRNA injections are unknown, and the benefits to this population (healthy children) is nil (9). It takes away from the mask optional and non-discriminatory messaging regarding policies mandating the prolonged masking of our children.
Medical or religious exemptions should be honored if coercive messaging and mandates continue for masking/testing /vaccines, especially if they are discriminatory. (9) In his article, “Vaccine Exemption Letter for a 16-Year-Old Camp Counselor”, Dr. Kory writes a vaccine exemption that provides an example of what informed consent looks like—in this case for a vaccine exemption. There have been challenges and obstacles to mask, testing, and vaccine exemptions within the school and college communities.
I shudder to think that our children could be back into mandatory prolonged masking this fall if our schools continue to implement the same failed policies under the guidance of the local health boards and the CDC, but it would not surprise me given the experiences over the last 2 years. This time, it will be knowing of the harm it has caused. Will our health boards and school boards continue to follow the CDC guidelines despite increasing numbers of parents being equipped with information to push back knowing how these policies harm our children? When there is the potential for harm, there is the need for choice. Giving choice to parents should appease parents on both sides of this issue. For those parents who feel that masking and “vaccinating” their child will keep them safe, that is their decision. If they truly believe this, then they should feel assured that their children is protected by the mask and “vaccine.” As a mother and physician, I am asking for the same opportunity to protect my children FROM the mask and “vaccine” while proceeding with other options that I believe are safer and more effective in mitigating COVID 19 risk.
Sincerely, Dana H. Granberg-Nill, MD FAAFP
References:
1. Children, Covid and the Urgency of Normal. Version 2/18/2022. An advocacy toolkit used for parents, students, mentors, teachers, and administrators. www.urgencyofnormal.com.
5. CDC Wants its COVID Regimen Made Permanent. Jeffrey Tucker. The Epoch Times Viewpoint. June 10, 2022.
6. The Dangers of Masks. Paul Alexander, MSc, PhD, Howard Tenenbaum, DDS, PhD, Parvez Dara, MD, MBA. 11/11/2022. American Institute for Economic Research. https://www.aier.org/article/the-dangers-of-masks/
12. Urgencyofnormal.com -Official website and source of the Toolkit, panelists bios, etc.
13. Emails Confirm Why CDC Changed Definitions of Vaccine, Vaccinated. Zachary Stieber. July 11, 2022.
14. Correlation Between Mask Compliance and COVID-19 Outcomes in Europe. Alexander Muacevic and John R Adler. NIH, National Library of Medicine. Apr; 14(4), 2022.
15. Follow the Money: Blood Money in U.S. Schools. Summary Brief, Revised July 8, 2022. AJ Depriest and TN Liberty Network.
18. Providone-Iodine Use in Sinonasal and Oral Cavitis: A Review of Safety in the COVID-19 Era. Ear, Nose and Throat Journal. Samantha Frank, M.D., Joseph Caproiotti, M.D. and Seth Brown, MD, MBA. June 10, 2020.
19. Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines. American Journal of Therapeutics. 2021 Andrew Bryant, MSc, Theresa Lawrie, MBBCH, PhD, Therese Dowswell, PhD, Edmund Fordham, Phd, Scott Mitchell, MBChB, MRCS, Sarah Hill, Phd, and Tony Tham, MD, FRCP. www.americantherapeutics.com
20. Clinical Infectious Diseases Reinfections vs Breakthrough Infections: Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Naturally Acquired Immunity versus Vaccine-induced Immunity, Reinfections versus Breakthrough Infections: A Retrospective Cohort Study. Clinical Infectious Disease 2022. Sivan Gazit,1,2, Roei Shlezinger,1 Galit Perez,2 Roni Lotan,2 Asaf Peretz,1,3 Amir Ben-Tov,1,4 Esma Herzel,2 Hillel Alapi,2 Dani Cohen,4 Khitam Muhsen,4Gabriel Chodick,2,4 and Tal Patalon
21. 'UK Gov. quietly published a report confirming the Vaccinated account for 94% of all COVID-19 Deaths since April, 90% of which were Triple/Quadruple Jabbed' Paul Alexander. July 11, 2022. .
22. Adverse effects of COVID-19 vaccines and measures to prevent them. PubMed.gov NIH National Library of Medicine. Kenji Yamamoto. Virol J. 2022.
23. Judge scraps 75-year FDA timeline to release Pfizer vaccine safety data, giving agency eight months. Kaelan Deese, Supreme Court Reporter. January 07, 2022 10:39 AM
28. Regular use of ivermectin as prophylaxis for COVID-19 led up to92% reduction in COVID-19 mortality rate in a dose-response manner: results of a prospective observational study of a strictly controlled population of 88,012 subjects among 223,128 participants. Lucy Kerr, et al. Preprint July 2022. Research Gate.
29. Nursing student sues school after being denied a COVID-19 vaccination exemption. Clark Kauffman. Iowa Dispatch. July 25, 2022.
Appendix:
Missouri Driver’s License Office May of 2022. This sign was present long after it was widely known that “vaccination” did not prevent transmission.
The Kauffman Center of Performing Arts had instituted a policy of proof of vaccination for attendees even after the CDC confirmed that the “vaccination” did not prevent transmission. It is no longer required.
👏 Yes, yes, yes! Thank you, Dr. Granberg-Nill, for being a voice of truth! Thank you for advocating for our children! This needs to be shared far and wide! We all need to pass this on to our legislators, school boards and health boards!!!




Well done, Dr. Granberg! Your courage to speak truth is sincerely appreciated!
👏 Yes, yes, yes! Thank you, Dr. Granberg-Nill, for being a voice of truth! Thank you for advocating for our children! This needs to be shared far and wide! We all need to pass this on to our legislators, school boards and health boards!!!